
Last update and review: February 5, 2020.
A short summary.
This article was written around April 2020 and reflects our understanding of the situation at that time. For a more recent update, check the article linked below as well as other more recent articles on our website.
Our understanding of the situation with COVID-19 as of April and May 2020.
Containing COVID-19 did not work. Fortunately, only a minority of the population turned out to be “susceptible” to SARS-CoV-2. Indeed, the curves describing the number of cases peaked before a substantial proportion of the population could get infected with SARS-CoV-2. So, the COVDI-19 epidemic turned out to be not as bad as the propaganda and incompetent bureaucrats claimed.

However, the eradication of the SARS-CoV-2 virus is unlikely. This means that the infection will most likely continue to spread albeit at low basal levels. The disease itself, COVID-19, is serious, and the risk to get infected with it will remain real for the months and years to come. Are you ready to deal with it? Do you know enough to minimize the damage?
Due largely to the incompetence of medical doctors, COVID-19 mortality rates are around 20% in some hospitals.
We now also know that COVID-19 mortality rates can be catastrophic. Below, you can find European countries ranked by their “official” COVID-19 mortality rates. “Official” means that it is based on the data that the countries submit to the WHO. The original WHO report from April 10, 2020, that we used to calculate these mortality rates is also inserted below.
As you can see, France holds the gruesome record with a 14.28% COVID-19 mortality rate.

There is another piece of data from France. The figure below was shared by one of the more competent medical teams, also in France, in the area of the city of Marseille. You can see the figure below that in some administrative areas of France, called “departments”, COVID-19 mortality rates are around 20%. This shows and abysmal incompetence of the medical doctors there.

The probability to get infected with SARS-CoV-2 remains high.
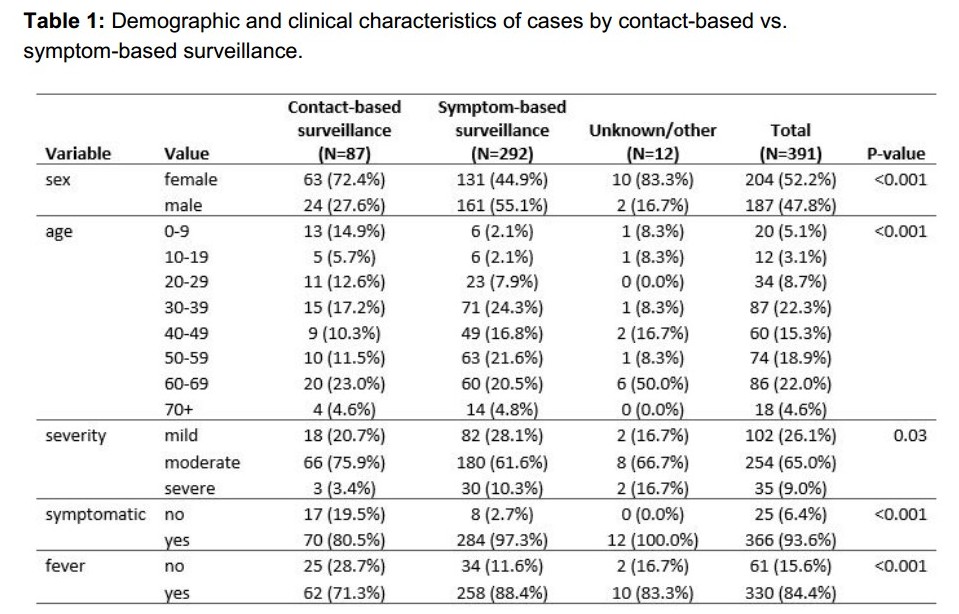
From a study from China (1), we know that only 17% of the infected had no symptoms (see the table below). A popular opinion that a vast majority of SARS-CoV-2 positive people are asymptomatic is incorrect. Among those who test positive on a PCR test for SARS-CoV-2, between 60% and 80% will have symptoms.
We also know that an infection with SARS-CoV-2 virus is not that benign even in healthy and young people. Another piece of data below from a paper in pre-print (2) shows that among 1061 patients treated for COVID-19 at a French hospital, only 34% had normal lungs on CT scan. This means that in 66% of the patients, the lungs were affected by the disease. This, despite the average relatively young age of these patients: “the mean age was 43.6 years old and 492 were male (46.4%)”. See a snapshot of the relevant part of the table from the study (2) below.

Are you ready for COVID-19?
We know that COVID-19 mortality rate can be as low as 2% in Germany (as of April 10, 2020). And even lower in some hospitals where the medical teams are competent. But a hospital near you may have an incompetent medical team. For example, the New York City area is a very bad place to be if you are a COVID-19 patient. Here is some horrifying statistics form a very recent study on 5700 patients in the New York City area.
Richardson et al., 2020 (3):
Outcomes were assessed for 2634 patients, 553 (21%) (of them) died.
Mortality for those requiring mechanical ventilation was 88.1%.
There is a degree of incompetence even in the phrase “those requiring mechanical ventilation”. To illustrate this, we will cite Martin J. Tobin, MD, who is an experienced pulmonologist and an author of books and articles on mechanical ventilation and intensive care (4):
Only a small proportion of patients—largely those in a cardiac arrest situation—“require” mechanical ventilation. In most instances, mechanical ventilation is instituted preemptively out of fear of an impending catastrophe.



In your geographic area, you may not receive the appropriate treatment or a timely treatment. If your disease takes a serious course, you again can be exposed to medical errors.
So, the risk of a poor outcome of COVID-19 is real even for relatively healthy and young people. But there are things that can be done to DELAY the moment of time when you get infected and to REDUCE the viral load that you may get at the moment of infection. A lower viral load may have a positive influence on the course of the disease.
As already mentioned at the beginning of this article, by the end of April, 2020, in a majority of countries, the curves depicting new COVID-19 cases had already peaked. And it happened before any substantial proportion of the population could get infected. We can conclude, that only a minority of the population is “susceptible” to SARS-CoV-2. This means that in the case of SARS-CoV-2, like in the case of many other viruses, there is no need for 70% of the population to get infected or be vaccinated to get to a “herd immunity”. The “susceptible” will get infected and will become “recovered”. The “non-susceptible” or “less susceptible” will not get infected.


An update from June 11, 2020: The following sentence from the May 5, 2020, version, is not entierly applicable to SARS-CoV-2: “Soon, there is a “herd immunity”. Indeed, the immunity to common human coronaviruses is not permanent. People who were infected in the past are NOT protected against future infections with the same virus. The hope is that second and the following infections with SARS-CoV-2 will be less severe than the first one. This, however, has not been shown yet.
An update from June 11, 2020: There are several countries where the COVID-19 epidemic was successfully “eliminated”. Switzerland is one such example. The number of new daily COVID-19 cases in Switzerland is around 10 as of early June, 2020. But in many other countries, COVID-19 became a chronic problem. Belarus and Singapore are two good example of this. About 0.2% of the population in Belarus and Singapore are infected with SARS-CoV-2 at any given time and the effective reproductive number is around 1.



The best strategy remains to avoid getting infected.
If, however, you do get infected with SARS-CoV-2 despite all your precautions, you need to be ready to get timely and appropriate treatment. There are “cures” that work and there are remedies that should help to minimize the impact of COVID-19. There are also steps that you may want to undertake to improve your health in general in order to be in better shape the day you catch the SARS-CoV-2 virus.
A consulting program: COVID-19 preparedness.
You can consult with us if you need support with the above. In this consultation, we can review your blood markers and other biomarkers. We can check if your understanding of COVID-19 is up to date with the most recent data and analysis. We can help you to adjust and finetune your preventive measures. We can also interact with your medical practitioner to make sure he or she is aware of the latest findings and research on COVID-19.
Selected references:
1. Bi (Qifang) et al. “Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 cases and 1,286 of their close contacts.” (2020) medRxiv preprint (was not yet peer-reviewed) https://doi.org/10.1101/2020.03.03.20028423
Accessed on April 11, 2020.
2. The abstract and the summary table of a paper by the IHU Mediterranee Infection, Marseille, paper on the treatment of 1061 COVID-19 patients. (2020).
A pre-print slides available at https://www.mediterranee-infection.com
Accessed on April 13, 2020.
3. Richardson et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA. doi:10.1001/jama.2020.6775
Published online April 22, 2020.
4. Tobin M.J., AJRCCM Articles in Press. Published April 13, 2020, (pre-print).
5 Comments